🧑🏫Anatomy
After this section, you should be able to
- ✅ Describe upper-extremity venous anatomy.
- ✅ Distinguish veins and venules from other important structures on ultrasound.
- ✅ Evaluate vessel suitability by analyzing its characteristics, dimensions and configuration.
🧑🏫Anatomy
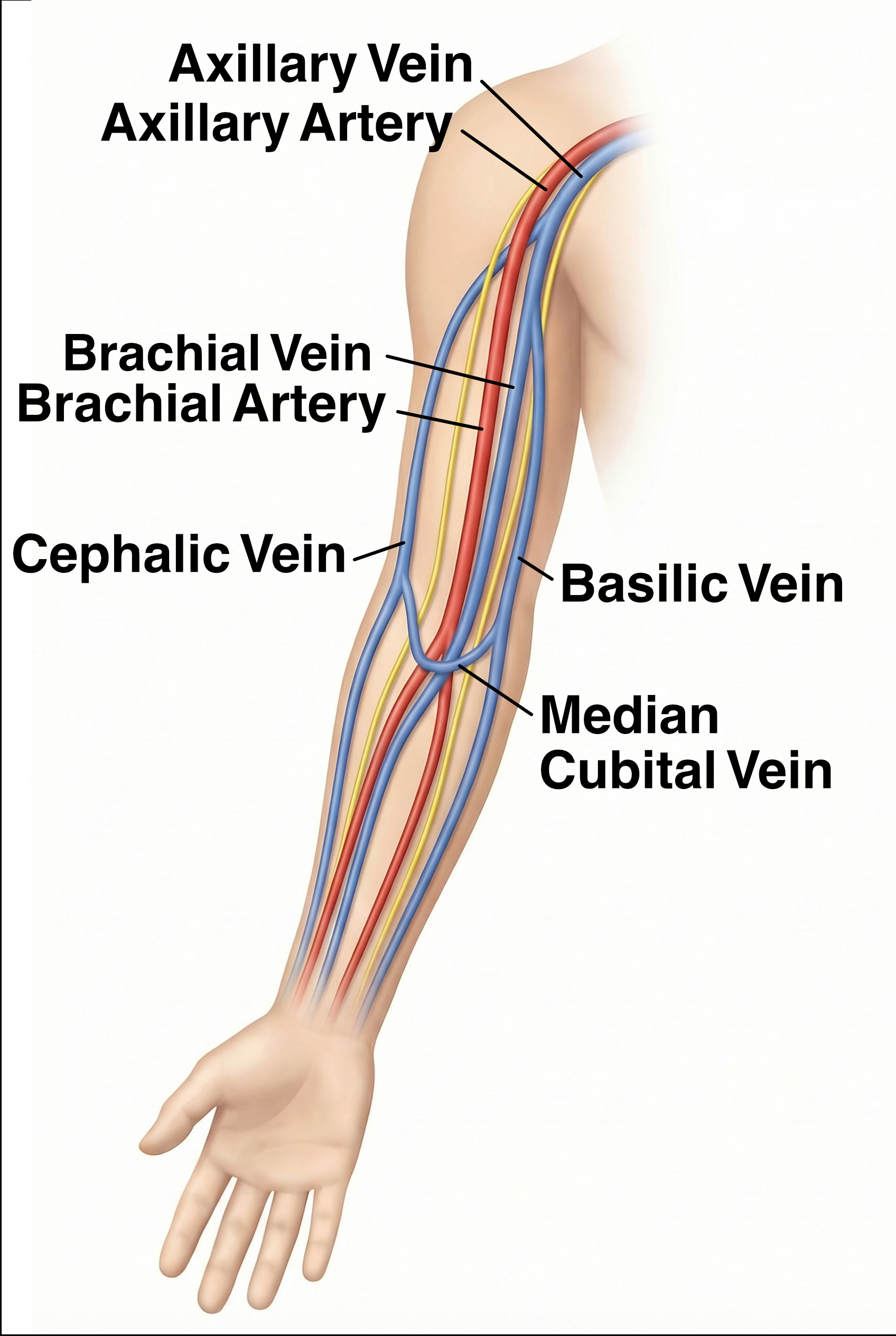
Veins that are suitable for ultrasound-guided cannulation are mostly found in the upper limbs on the volar surface. The simplified regional anatomy is described as follows:
- Cephalic Vein
- The Cephalic vein originates at the anatomical snuffbox and run along the radial surface of the forearm.
- It ascends the volar surface and communicate with the basilic vein via the median cubial vein at the elbow.
- It continues cephalad before joining the axillary vein.
- Basilic Vein
- The Basilic vein originates from the ulna volar aspect of the formarm and continue cephalad.
- It communicates with the cephalic vein via the medial cubital vein at the antecubital fossa.
- It drains into the brachial vein in the upper arm to form the axillary vein
- Median Cubital Vein
- The Median cubital vein is often the largest superficial vein of the upper arm.
- It connects the basilic and cephalic vein at the antecubital fossa.
- This vein is large, superficial and easily palpable but it can be tortorous and is prone to obstruction by elbow flexion.
- Brachial Vein
- The Brachial Vein is a deep vein that run deep to the muscles from forearm to upper arm.
- It runs along the brachial artery and joins the basilic vein to become axillary vein at the axilla.

🤔Considerations
The volar aspect of the forearm is a preferrable starting point, followed by basilic vein and the cephalic vein in the upper arm. There are several aspects for consideration when deciding a target site for cannulation, including vessel characteristics, location, depth and adjacent structures. Do not worry about the ultrasound images shown for illustration here yet, you will learn the skills to use and interpret ultrasound images in subsequent chapters.
⭐️Characteristics
- Size: Determine if the size of the vessel is suitable for cannulation. A smaller vein is associated with lower success rate. The diameter of the catheter should be less than 45% of that of the vessel.
- Course: Trace the course of the vessel. It is more difficult to cannulate a tortorous vein than a straight one. The patency of the cannula may be compromised by compression and dislodgement.
- Patency: Check whether a thrombus is present in the vein lumen. An uncompressible vein with echogenic thrombus is not suitable for cannulation. A patent compressible vein is shown on the right side in the following clip.

📍Location
- The volar aspect of the forearm is a desirable site because the skin is usually flat and the soft tissue is thin, making it a more stable surface. The vasculature is also more superficial on the volar surface.
- Antecubital fossa is another common site for IV access. However, it is prone to flow obstrcuction and cannula dislodgement caused by joint movements. It is crucial to educate the patient to avoid unnecessary elbow flexion. Alternatively, avoid setting IV at this site, especially on a dominant arm.
📐Depth

- Travelling distance: At an angle of 45°, the travelling distance of a catheter is roughly 1.4 times the depth of the vessel, i.e. \( \frac{1}{sin 45°} \cong 1.4 \), measured from the skin surface to the anterior vessel wall. This factor increases as the angle decreases. At 30°, that distance become 2 times the depth, i.e. \( \frac{1}{sin 30°} = 2 \)
- Intravascular placement: At least 2/3 of the catheter should be intravascular to reduce extravasation and dislodgement. In other words, the above travelling distance is only 1/3 of the recommended catheter length.
Combining the above estimations: $$Min. Length = Depth \times \frac{1.4}{1/3}$$ $$Min. Length \cong Depth \times4$$
- In adults, a catheter length of 1.75 inches (4.5cm) or more is usually adequate for most vessels within 1cm deep. The most ideal depth is 0.5cm. A vessel deeper than 1.5cm from the skin is considered unsuitable for peripheral IV access.
- The Brachial vein is a deep vessel, it should be used only as a last resort if all the superficial veins are unavailable or unsuitable.
⚠️Adjacent structures
- One should look for structures near the target vessel before deciding which vessel to use. The few locations listed below require more cautions than others. You will learn how to identify structures in the POCUS skills section.
- The wrist is rich of nerve bundles running close and parallel to veins. The risk of inadverdent nerve injury is high. Attempts should not be made at the wrist.
- The Brachial vein often runs closely parallel to the brachial artery and the median nerve. Proceed with caution and identify the adjacent structures before cannulation.

🔄Recap
What is definition of a difficult IV Access?
When there are two or more of the followings:
- More than two attempts are required for successful cannulation.
- A prior history of difficult access or failed attempts.
- No visible or palpable veins after tourniquet application.
- Clinical risk factors such as obesity, chronic illness, edema, or IV drug use.
What is the Modified A-DIVA Scale?
The following items each worth one point on Modified A-DIVA Scale
- Known history of difficult IV access.
- Expectation of a failed first attempt or difficult access.
- Inability to palpate a vein.
- Inability to visualize a vein.
- Largest vein diameter < 3 mm.