⚙️Preparation
Objectives
After reading this section, you should be able to:
- ✅Apply infection control standards for ultrasound-guided IV cannulation.
- ✅Pick the appropriate equipment and catheter for IV access.
- ✅Apply the strategies to optimize the environment and patient and provider positioning during the procedure.
☣️Infection control
- Follow your institute’s protocol on the infection control patients with transmissible diseases or carrier status.
- For the procedure itself, use either clean techniques with alcohol swabs, medical gloves, and tegaderm for covering the probe, or aseptic technique involving sterile dressing sets, sterile gloves, as well as sterile probe covers, subject to availability or local practice.
⚒️Equipment
- Transducer: A linear probe is used for visualising superficial structures.
- Catheter: Use IV catheters with 1.75 to 2.5 inches (4.5-6cm) length. In most hospitals, it means a 20G cannula or larger.
- Other supplies: Sterile probe cover or Tegaderm, gloves, tourniquet, sterile ultrasound gel, and skin disinfectant.

💺Ergonomics
- Lighting: Ensure adequate lighting in the environment. Dim the overhead lights if necessary to reduce glare on the ultrasound screen, while ensuring the insertion site remains clearly illuminated with a procedure lamp or spotlight.
- Positioning: Adjust the height of the chair and/or stretcher, and the desk if any to optimise the orgonomics. An uncomfortable posture of yourself and the patient will reduce the success rate of IV access and increase the risk of physical strain or needle-stick injuries.
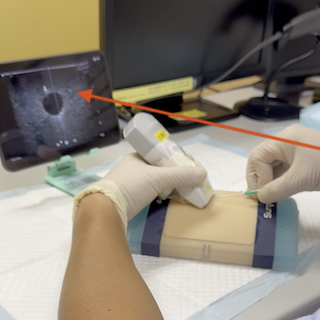
- Alignment: The patient, particularly the puncture site, the practitioner and the POCUS screen should be aligned in a single line of sight to minimize head turning and maintain hand-eye coordination. If you have to turn your neck more than 15–20 degrees to see the screen, your hand-eye coordination will suffer, increasing the risk of a needle drift.
- Stability: Ensure the patient’s arm is well-supported on a stable surface or arm cushion to prevent sudden movement during needle advancement.

🔄Recap
What score on the Modified A-DIVA Scale predicts a lower success rate without use of ultrasound?
A Score of 2 or above on the Modified A-DIVA Scale predicts a moderate or above difficulty. The cannulation success rate is 69% without ultrasound guidance. With ultrasound guidance, the success rate in these patient increase to above 71 to 75%
Which vessels in the upper limb are suitable for peripheral IV access with ultrasound?
The cephalic vein and the basilic vein are the first choice, particularly in the forearm. The median cubital vein is also suitable but caution is needed. The brachial veins are very deep and should be the last resort.